Chady El Tawil, Imane Chedid, Amy Bergeron, Isabelle Gagnon, Ilana Greenstone (Author)
Objectives: Return visits (RVs) to the emergency department (ED) has always been a major concern. RVs to the emergency department are a big burden on the healthcare system as its cost is higher than the cost of the initial visit. This review was performed to identify factors associated with risk of RVs to the pediatric ED.
Methods and Analysis: One researcher searched Medline, Embase, Cochrane Library and Web of Science. Studies were identified by using MeSH and keywords and included RVs to the pediatric ED up to 1 year a primary outcome. All studies were screened by two independent reviewers for eligibility and in case of disagreement, a meeting was held to discuss the problematic studies and a consensus was achieved.
Results: The search identified 539 reports from which 28 articles were included. Data was then extracted from the included studies according to a preset format. The exposures were grouped in 3 different groups: very probable, possible, and less likely.
As a result, young age, language barrier and high acuity were identified as very probable risk factors. Having a public insurance or with low income, patients with comorbidities and patients who had multiple previous ED visits were found to be possible risk factors for return visits.
Conclusion: Young age, high acuity and language barrier among others are risk factors for return visits to the pediatric ED. Physicians should be aware of these factors and have a low threshold for admission or a good discharge plan for patients with one or more factors.
Key Messages:
Ø What is already known on this topic – Return visits (RV) to the pediatric emergency department has always been a major concern and a big burden on the healthcare system as its cost is higher than the cost of the initial visit. The risk factors for RV vary widely.
Ø What this study adds – Young age, language barrier and high acuity were identified as very probable risk factors. Having a public insurance or with low income, patients with comorbidities and patients who had multiple previous ED visits were found to be possible risk factors for return visits.
Ø How this study might affect research, practice, or policy – Physicians should be aware of these factors and have a low threshold for admission or a good discharge plan for patients with one or more factors.
Introduction
Return visits (RVs) to the emergency department (ED) have always been a major concern. In fact, since the 1980s, emergency physicians recognized return visits, also known as bounce back visits, as a “red flag” for low quality of care [1]. In general, RVs to the emergency (ED) constitute an enormous burden on the healthcare system. For instance, on a financial level, the cost of a RV is higher than the cost of the initial visit [2]. Further, on a medical level, patients admitted to the Pediatric Intensive Care Unit (PICU) following a RV to the pediatric ED, are more likely to be put on a ventilator [3]. For these reasons, RVs have often been used as a quality metric in the pediatric ED [4].
As traditionally reported in many studies, a visit occurring within 72-hours of an index presentation for the same complaint is considered to be a RV because it reflects either an inadequate treatment or a missed diagnosis [5-7]. However, more recently, the 72-hour limit has been challenged by many as it might not mirror neither of both classifications (i.e., inadequate treatment or missed diagnosis) [8]. Indeed, some of the most common pediatric presentations to the ED, such as allergic reaction, asthma, fever, and bronchiolitis, can either deteriorate or have symptoms requiring a RV to the ED after more than 3 days, which in this case, doesn’t constitute a low quality of care. Longer time periods have also been proposed in adult EDs. For example, a recently published large retrospective study including more than one million adult ED RVs over 10 years used an upper limit of 14 days after the initial visit. The authors concluded that these patients should be identified early to avoid intensive care unit (ICU) admission during the RV [9].
Identifying risk factors leading to RVs could contribute to improved care for children presenting to pediatric EDs. An initial search performed in preparation for our study identified one literature review published in 2016 on the topic of risk factors and interventions that affected RVs to the pediatric ED [8]. This review concluded that mental health problems, younger age, acuity of illness, medical history of asthma, and social factors are risk factors for RVs. However, this review looked at studies published prior to November 2012 and identified only 6 studies looking at RVs ranging from 48 hours to 1 year. Also, as the authors mentioned in their study limitations’ section, they only investigated Medline without grading the reviewed studies for quality. Further, 3 out of the 6 studies were limited to a specific condition (2 included only patients with asthma and 1 included patients with mental health-related issues), limiting therefore the diversity of the collected data and hence its generalizability to the context of RVs.
To fill out the previous gap, we performed a systematic search and review to identify factors associated with risk of RVs to the pediatric ED in children of any age as defined by the authors in each article. As there is no true consensus on the delay where a subsequent visit would be considered a RV, we considered 1 year as a reasonable cutoff as considered in the previous review mentioned prior. However, no differentiation was made between RVs for the same problem and RVs for an unrelated complaint to the initial visit. We aimed to answer the following question: in pediatric patients of any age presenting to the emergency department, what risk factors on the first presentation would predict a RV within 1 year?
Materials and Methods
Search Strategy
The following databases were searched for relevant records on April 22 2021: Medline (via Ovid 1946 to 2021 April 21), Cochrane (via Wiley, from the Cochrane Database of Systematic Reviews, Issue 3 of 12, March 2021), Embase (via Ovid 1947 to 2021 April 21), and Web of Science (via Clarivate, Indexes SCI-EXPANDED, SSCI, A&HCI, CPCI-S, CPCI-SSH, BKCI-S, BKCI-SSH, ESCI, CCR-EXPANDED, & IC).
The search strategies designed by a librarian (AB) used text words and relevant indexing to identify records on risk factors for pediatric emergency readmission.
The final Medline strategy (Appendix 1) was adapted for all databases, with modifications to search terms and syntax as necessary. No language limits were applied.
Inclusion Criteria
The included studies were limited to randomized controlled trials (RCTs), controlled studies, systematic reviews, cohort studies, case control studies and cross-sectional studies written in English or French without any date limit for inclusion. Case reports and series were excluded. Also, studies looking into one diagnosis (like asthma, bronchiolitis…) were excluded because risk factors for RVs can be confounding factors and not true risk factors (for example, bronchiolitis is diagnosed in kids less than 12-24 months making young age a confounding factor), however, studies with a large scope of presentation and low risk for confounding factors (like trauma) were included.
No restriction was made on the past medical history, perinatal history, previous hospitalizations, medications, gender, acuity on presentation, medical interventions on the first visit, length of stay (LOS), left without being seen (LWBS), left against medical advice (AMA) or any other criteria. However, according to our search, these might be identified as risk factors for RVs.
Screening
All studies were screened by title first then by abstract by two independent reviewers (CET and IC). Duplicated studies in different databases were removed. Studies not satisfying the inclusion criteria were then excluded. Further, following an independent extraction of data, both reviewers compared results to reach a consensus.
Data extraction
Data were extracted by the two independent reviewers according to a predefined format (Table 1). Data points collected included the first author’s name, the study characteristics (type of study, date of publication, total number of RVs and country where the study was conducted), the timing of the RV (i.e., outcome) and the identified risk factors (i.e., exposures).
Results
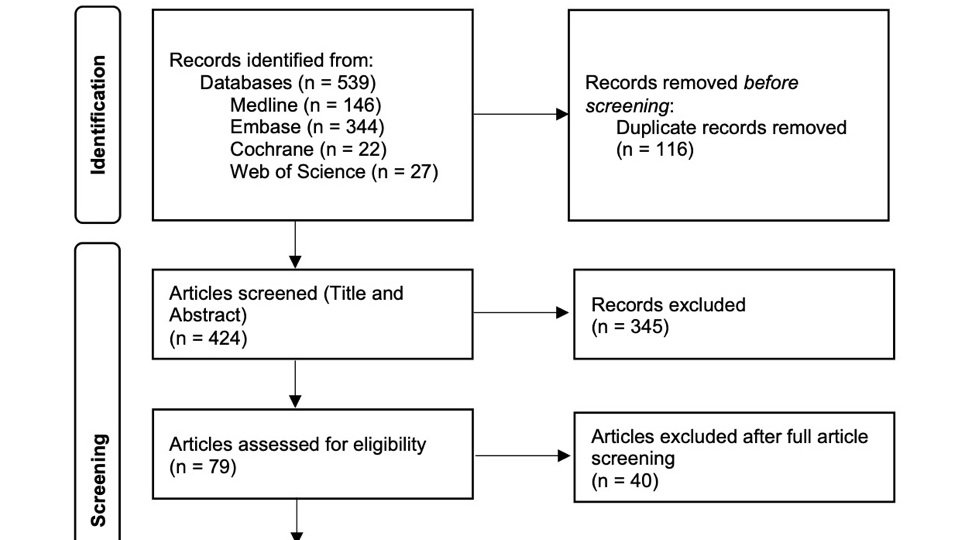
The initial search identified 539 articles (Figure 1).
After removal of duplicate studies and screening of titles and abstracts by the 2 independent reviewers, 79 articles were included. Forty reports were then excluded after full manuscript review by both reviewers. For the remaining articles, a meeting between the 2 reviewers and a consensus to include 28 articles was achieved [8, 10-36].
Data were then extracted from the included studies according to the preset format (Table 1). The data in italic format in the table represent a negative or neutral finding (for example, in Daymont et al. discharge heart rate was not found to affect RVs). The risk factors were then divided into 3 different groups according to how many times they were cited as there was no other practical way to weigh and compare the studies (Figure 2).
Discussion
This review identified multiple risk factors for RVs to the pediatric ED.
Young Age
Infant and young children were, by far, more likely to have a RV to the ED than older children and adolescents even though the definition of young age was different between studies ranging from younger than 1 year to younger than 5 years. While these RVs might be due to progression of the disease, such as bronchiolitis, in this age group, clear discharge instructions and explanation of signs of deterioration were found to be a protective factor against unnecessary RVs [37].
Language
Language barrier between patients and healthcare providers has been associated with increased pediatric ED visit length of stay and resource utilization in addition to increased RVs [38, 39 ]. With the increased number of refugees worldwide, language barrier is becoming more relevant and the need for multilingual healthcare professionals is constantly increasing [40].
High Acuity
Pediatric patients who are sicker at triage are more likely to be admitted especially in a crowded ED [41]. If those patients with higher acuity are discharged from the ED, they are more likely to bounce back. Physicians should probably maintain a low threshold for admission at the time of the initial visit [42].
Other Risk Factors
This review identified more risk factors like patients with public insurance or with low income, patients with comorbidities and patients who had multiple previous ED visits. How to classify a RV after LWBS and, to a lesser extent AMA, is controversial. It might be considered as the first visit and not a RV since the patient was not assessed by the physician and/or did not receive the proper management for their condition.
Studies Quality and Limitations
Most of the studies were retrospective (86%) with only two prospective studies, one of which was a planned secondary analysis of a prospective cohort. The majority were North American studies (68%), limiting therefore the diversity and generalizability of our findings. The primary outcome was different across the articles: although it was mostly risk factors for RVs, there was a big discrepancy in the risk factors studied as some of the risk factors were frequent, cited up to 16 times (age), while others were rare, with only 2 citations (season).
Due to these limitations and the heterogeneity of the articles, the wide variety of variables, as well as a lack of a true definition of the outcome (RV ranged from 48 hours to 1 year), and of a grading system for most observational studies in this review, a systematic review and meta-analysis were not feasible. Therefore, a systematic search and review was conducted [43]. Most of the articles were also retrospective and arguably have low weight to form a robust meta-analysis. In addition, RV can have different expressions ranging from unplanned revisits to readmissions visits, among others. This means that despite the comprehensive search (Appendix 1), we might have missed some articles. However, this would probably not affect the results significantly as there is a visible consensus between the different studies that were included. Also, using such a wide time limit of one year and not differentiating between RVs for the same problem and RVs for an unrelated complaint to the initial visit might have influenced the results however, most studies did not specify if the RV complaint was different from the initial visit. Finally, this review did not look at the disposition of patients during the RV as the RV outcome can range from discharging the patient home to admission to wards/ICU to mortality and would obviously affect the weight and importance of each identified risk factor.
Conclusion
Young age, high acuity at presentation and language barrier, among others, are risk factors for return visits to the pediatric ED. Physicians should be aware of these factors and have a low threshold for admission or a good discharge plan for patients with one or more factors to improve quality care in the pediatric ED. While pediatric ED overcrowding is a burden worldwide, such studies can help decompress the EDs by identifying high risk patients and reducing RVs.
Declarations
Author contributions: All authors contributed equally and validated the final version of record.
Conflicts Of Interest: The Author(s) declare(s) that there is no conflict of interest.
Funding: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Registration: No registration applicable
Data availability statement: The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethical approval: Ethical approval for this study was not required.
References
1. Lerman B, Kobernick MS. Return visits to the emergency department. J Emerg Med. 1987 Sep 1;5(5):359–62. https://doi.org/10.1016/0736-4679(87)90138-7.
2. Duseja R, Bardach NS, Lin GA, Yazdany J, Dean ML, Clay TH, et al. Revisit Rates and Associated Costs After an Emergency Department Encounter. Ann Intern Med. 2015 Jun 2;162(11):750–6. https://doi.org/10.7326/M14-1616.
3. Chiang CY, Cheng FJ, Huang YS, Chen YL, Wu KH, Chiu IM. ICU admission following an unscheduled return visit to the pediatric emergency department within 72 hours. BMC Pediatrics. 2019 Aug 2;19(1):268. https://doi.org/10.1186/s12887-019-1644-y.
4. Ostrow O, Zelinka A, Shim A, Azmat SK, Masood S, Chartier LB. Pediatric Emergency Department Return Visits: An Innovative and Systematic Approach to Promote Quality Improvement and Patient Safety. Pediatr Emerg Care. 2020;36(12):e726–31. https://doi.org/10.1097/PEC.0000000000001999.
5. Ko M, Lee Y, Chen C, Chou P, Chu D. Incidence of and Predictors for Early Return Visits to the Emergency Department: A Population-Based Survey. Medicine. 2015;94(43):e1770. https://doi.org/10.1097/MD.0000000000001770.
6. Benbassat J, Taragin M. Hospital Readmissions as a Measure of Quality of Health Care: Advantages and Limitations. Arch Intern Med. 2000 Apr 24;160(8):1074–81. https://doi.org/10.1001/archinte.160.8.1074.
7. Trivedy CR, Cooke MW. Unscheduled return visits (URV) in adults to the emergency department (ED): a rapid evidence assessment policy review. Emerg Med J. 2015 Apr 1;32(4):324. https://doi.org/10.1136/emermed-2013-202719.
8. Tran QK, Bayram JD, Boonyasai RT, Case MA, Connor C, Doggett D, et al. Pediatric Emergency Department Return: A Literature Review of Risk Factors and Interventions. Pediatr Emerg Care. 2016;32(8):570–7. https://doi.org/10.1097/PEC.0000000000000876.
9. Aaronson E, Jansson P, Wittbold K, Flavin S, Borczuk P. Unscheduled return visits to the emergency department with ICU admission: A trigger tool for diagnostic error. Am J Emerg Med. 2020 Aug 1;38(8):1584–7. https://doi.org/10.1016/j.ajem.2019.158430.
10. Ehwerhemuepha L, Yu PT, Guner YS, Wallace E, Feaster W. A Nested Mixed Effects Multicenter Model Examining the Risk Factors for Pediatric Trauma Return Visits Within 72 Hours. J Surg Res. 2021 Jan 1;257:370–8. https://doi.org/10.1016/j.jss.2020.08.021.
11. Pershad J, Jones T, Harrell C, Ajayi S, Giles K, Cross C, et al. Factors Associated With Return Visits at 7 Days After Hospital Discharge. Hosp Pediatr. 2020 Apr 1;10(4):353–8. https://doi.org/10.1542/hpeds.2019-0207.
12. Türe E, Yazar A. Retrospective Evaluation of Return Visits to the Paediatric Emergency Department. Eurasian J Emerg Med. 2020 Jun 22;19(2):115–20. https://doi.org/10.4274/eajem.galenos.2019.68926.
13. Drouin O, D’Angelo A, Gravel J. Impact of wait time during a first pediatric emergency room visit on likelihood of revisit in the next year. Am J Emerg Med. 2020 May 1;38(5):890–4. https://doi.org/10.1016/j.ajem.2019.07.005.
14. Daymont C, Balamuth F, Scott HF, Bonafide CP, Brady PW, Depinet H, et al. Elevated Heart Rate and Risk of Revisit With Admission in Pediatric Emergency Patients. Pediatr Emerg Care. 2021 Apr;37(4):e185–91. https://doi.org/10.1097/PEC.0000000000001552.
15. de Vos-Kerkhof E, Geurts DHF, Steyerberg EW, Lakhanpaul M, Moll HA, Oostenbrink R. Characteristics of revisits of children at risk for serious infections in pediatric emergency care. Eur J Pediatr. 2018 Apr 1;177(4):617–24. https://doi.org/10.1007/s00431-018-3095-0.
16. Kim BS, Kim JY, Choi SH, Yoon YH. Understanding the characteristics of recurrent visits to the emergency department by paediatric patients: a retrospective observational study conducted at three tertiary hospitals in Korea. BMJ Open. 2018 Feb 1;8(2):e018208. https://doi.org/10.1136/bmjopen-2017-018208.
17. Michelson KA, Lyons TW, Bachur RG, Monuteaux MC, Finkelstein JA. Timing and Location of Emergency Department Revisits. Pediatrics. 2018 May 1;141(5):e20174087. https://doi.org/10.1542/peds.2017-4087.
18. Meyer-Macaulay CB, Truong M, Meckler GD, Doan QH. Return visits to the pediatric emergency department: A multicentre retrospective cohort study. CJEM. 2018;20(4):578–85. https://doi.org/10.1017/cem.2017.40.
19. Ruttan T, Lawson KA, Piper K, Wilkinson M. Risk Factors Associated With Emergency Department Return Visits Following Trauma System Discharge. Pediatr Emerg Care. 2018;34(3):202–7. https://doi.org/10.1097/PEC.0000000000001182.
20. Hu YH, Tai CT, Chen SCC, Lee HW, Sung SF. Predicting return visits to the emergency department for pediatric patients: Applying supervised learning techniques to the Taiwan National Health Insurance Research Database. Comput Methods Programs Biomed. 2017 Jun 1;144:105–12. https://doi.org/10.1016/j.cmpb.2017.03.022.
21. Kilicaslan O, Sönmez FT, Gunes H, Temizkan RC, Kocabay K, Saritas A. Short Term Unscheduled Revisits to Paediatric Emergency Department - A Six Year Data. J Clin Diagn Res. 2017 Mar 1;11(3):SC12-SC15. https://doi.org/10.7860/JCDR/2017/25098.9484.
22. Samuels-Kalow ME, Stack AM, Amico K, Porter SC. Parental Language and Return Visits to the Emergency Department After Discharge. Pediatr Emerg Care. 2017 Jun;33(6):402-404. https://doi.org/10.1097/PEC.0000000000000592.
23. Wilson PM, Florin TA, Huang G, Fenchel M, Mittiga MR. Is Tachycardia at Discharge From the Pediatric Emergency Department a Cause for Concern? A Nonconcurrent Cohort Study. Ann Emerg Med. 2017 Sep;70(3):268-276.e2. https://doi.org/10.1016/j.annemergmed.2016.12.010.
24. Goh GL, Huang P, Kong MC, Chew SP, Ganapathy S. Unplanned reattendances at the paediatric emergency department within 72 hours: a one-year experience in KKH. Singapore Med J. 2016;57(6):307-13. https://doi.org/10.11622/smedj.2016105.
25. Schneider M, Chen C, Menoch M, Levasseur K. Primary language and return visits in the pediatric emergency department. SAEM Annual Meeting Abstracts. Acad Emerg Med. 2016 May 1;23(S1):S103-4. https://doi.org/10.1111/acem.12974.
26. de Vos-Kerkhof E, Geurts DH, Wiggers M, Moll HA, Oostenbrink R. Tools for 'safety netting' in common paediatric illnesses: a systematic review in emergency care. Arch Dis Child. 2016 Feb;101(2):131-9. https://doi.org/10.1136/archdischild-2014-306953.
27. Saunders N, To T, Parkin P, Guttmann A. The relationship between immigrant status and pediatric emergency department return visits. Paediatrics and Child Health (Canada). 2015;20:e93. https://doi.org/10.1093/pch/20.5.e93.
28. Sung SF, Liu KE, Chen SC, Lo CL, Lin KC, Hu YH. Predicting Factors and Risk Stratification for Return Visits to the Emergency Department Within 72 Hours in Pediatric Patients. Pediatr Emerg Care. 2015 Dec;31(12):819-24. https://doi.org/10.1097/PEC.0000000000000417.
29. Gallagher RA, Porter S, Monuteaux MC, Stack AM. Unscheduled return visits to the emergency department: the impact of language. Pediatr Emerg Care. 2013 May;29(5):579-83. https://doi.org/10.1097/PEC.0b013e31828e62f4
30. Samuels-Kalow ME, Stack AM, Amico K, Porter SC. The association between parental language and 72-hour revisits following pediatric emergency department discharge. SAEM Annual Meeting Abstracts. Acad Emerg Med. 2013 May 1;20(s1):S188. https://doi.org/10.1111/acem.12115.
31. Gaucher N, Bailey B, Gravel J. Impact of physicians' characteristics on the admission risk among children visiting a pediatric emergency department. Pediatr Emerg Care. 2012 Feb;28(2):120-4. https://doi.org/10.1097/PEC.0b013e318243f8e0.
32. Reinke DA, Walker M, Boslaugh S, Hodge D 3rd. Predictors of pediatric emergency patients discharged against medical advice. Clin Pediatr (Phila). 2009 Apr;48(3):263-70. https://doi.org/10.1177/0009922808323109.
33. Costabel S, Piccotti E, Sartini M, Magnani M, Di Pietro P. Return visits to the Paediatric Emergency Department: first analysis in Italy. J Prev Med Hyg. 2008 Dec;49(4):142-7. https://doi.org/10.15167/2421-4248/jpmh2008.49.4.133
34. Goldman RD, Ong M, Macpherson A. Unscheduled return visits to the pediatric emergency department-one-year experience. Pediatr Emerg Care. 2006 Aug;22(8):545-9. https://doi.org/10.1097/01.pec.0000230553.01917.05.
35. LeDuc K, Rosebrook H, Rannie M, Gao D. Pediatric emergency department recidivism: demographic characteristics and diagnostic predictors. J Emerg Nurs. 2006 Apr;32(2):131-8. https://doi.org/10.1016/j.jen.2005.11.005.
36. Alessandrini EA, Lavelle JM, Grenfell SM, Jacobstein CR, Shaw KN. Return visits to a pediatric emergency department. Pediatr Emerg Care. 2004 Mar;20(3):166-171. https://doi.org/10.1097/01.pec.0000117924.65522.a1.
37. Navanandan N, Schmidt SK, Cabrera N, Topoz I, DiStefano MC, Mistry RD. Seventy-two-hour Return Initiative: Improving Emergency Department Discharge to Decrease Returns. Pediatr Qual Saf. 2020 Sep 25;5(5):e342. https://doi.org/10.1097/pq9.0000000000000342.
38. Hampers LC, Cha S, Gutglass DJ, Binns HJ, Krug SE. Language barriers and resource utilization in a pediatric emergency department. Pediatrics. 1999 Jun;103(6):1253-6. https://doi.org/10.1542/peds.103.6.1253.
39. Zamor R, Byczkowski T, Zhang Y, Vaughn L, Mahabee-Gittens EM. Language Barriers and the Management of Bronchiolitis in a Pediatric Emergency Department. Acad Pediatr. 2020 Apr;20(3):356-363. https://doi.org/10.1016/j.acap.2020.01.006.
40. Hampers LC, McNulty JE. Professional interpreters and bilingual physicians in a pediatric emergency department: effect on resource utilization. Arch Pediatr Adolesc Med. 2002 Nov;156(11):1108-13. https://doi.org/10.1001/archpedi.156.11.1108.
41. Doan Q, Wong H, Meckler G, Johnson D, Stang A, Dixon A, et al. The impact of pediatric emergency department crowding on patient and health care system outcomes: a multicentre cohort study. CMAJ. 2019 Jun 10;191(23):E627-35. https://doi.org/10.1503/cmaj.181426.
42. Al-Qahtani MH, Yousef AA, Awary BH, Albuali WH, Al Ghamdi MA, AlOmar RS, et al. Characteristics of visits and predictors of admission from a paediatric emergency room in Saudi Arabia. BMC Emerg Med. 2021 Jun 21;21(1):72. https://doi.org/10.1186/s12873-021-00467-7.
43. Grant MJ, Booth A. A typology of reviews: an analysis of 14 review types and associated methodologies. Health Info Libr J. 2009 Jun;26(2):91-108. https://doi.org/10.1111/j.1471-1842.2009.00848.x.